Ashok Balasubramanyam, MD, Chair of ABIM’s Endocrinology, Diabetes & Metabolism Board
ABIM’s new Longitudinal Knowledge Assessment (LKATM) for Maintenance of Certification (MOC) launches in January 2022, and will offer a re-imagined assessment experience designed to meet the needs of today’s practicing physician.
Ashok Balasubramanyam, MD, Chair of ABIM’s Endocrinology, Diabetes & Metabolism Board is planning to participate in the LKA, and shared some background on why he is choosing it instead of the traditional, 10-year MOC exam.
“I’ve been really excited to see the LKA develop over the past several years,” said Dr. Balasubramanyam. “The care and thinking behind it has really been an eye opener for me. For example, there’s a very detailed process for creating exam blueprints for the 10-year exam, which is also being done for the LKA. That means no matter which exam a physician chooses, it will be of high quality and relevancy to physicians in their field.”
Dr. Balasubramanyam cited how specific features of the LKA – such as the ability to take questions on an ongoing basis – fits better with the way he learns and keeps his medical knowledge current.
“When I took the 10-year exam I really needed to cram, which I didn’t like as it caused a lot of stress. I also came to realize that once the exam was over, I didn’t feel that I retained most of what I had studied,” he said.
Both the 10-year MOC exam and LKA provide physicians with feedback on their performance, but there are important differences between the two.
“With the 10-year exam there was an opportunity to go back and look at my exam performance via the score report ABIM provides, which I did find helpful. But with LKA you’re getting real-time feedback – after most questions you’ll know immediately if you got it right or wrong, and will be provided with a rationale for why along with a few relevant references. That makes the LKA a good learning experience as well as an assessment, and I can see how that will benefit me and my practice.”
Another difference between the LKA and 10-year exam is the time of year physicians engage in the assessment. Physicians can register to take a 10-year exam that occurs in the Spring or Fall administrations, and can wait until as late as mid-August to sign up.
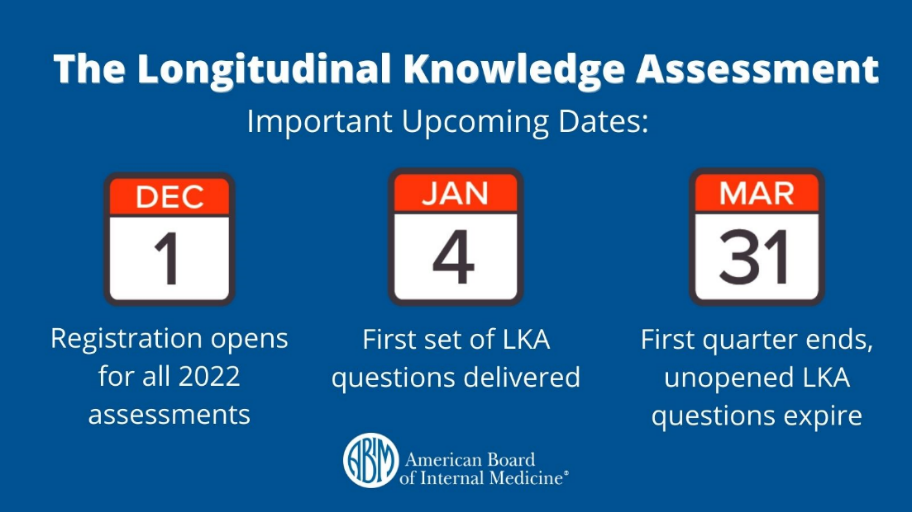
But with the LKA, physicians should enroll and engage as early as possible as the first quarter’s questions will be delivered 1/4/22. Any unopened questions expire at the end of each quarter, meaning that if a physician enrolls after 3/31/22, the first quarter’s questions will have already expired and count against the 100 questions a physician can choose not to open over 5 years.
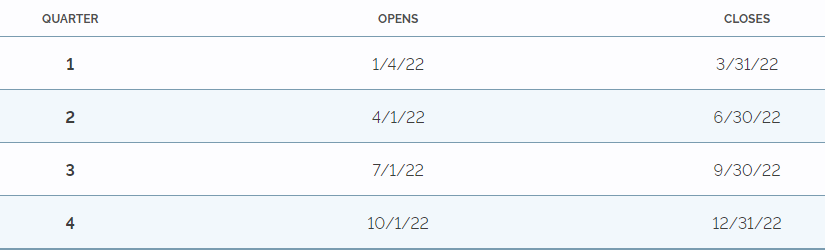
2022 LKA Question Release Schedule
Dr. Balasubramanyam shared a number of other LKA features he was looking forward to, such as not needing to schedule an appointment or go to a test center. With the LKA physicians can take questions on their own devices, and in their home, office, or wherever they’re most comfortable and can focus. He also appreciated the ability to use the same medical resources he uses in practice when taking questions – anything except another person.
“I have a lot of apps on my phone I use regularly to look things up when I see patients or in consultation with colleagues, but sometimes I rely on a simple Google search. As long as I know I’m accessing a reliable source, I feel confident in the information,” he said.
As for how he plans to utilize external resources, Dr. Balasubramanyam mentioned some of the feedback he’s heard from colleagues about the four-minute time limit for each question.
“Four minutes is actually more time than people might think. And it’s important to remember in practice we don’t have an unlimited amount of time with our patients or to respond to a colleague. But that’s also why there’s a time bank physicians can utilize if they need a little more time on a specific question.”
Enrollment for all ABIM MOC assessments – including the LKA – opens 12/1/21. Learn about eligibility, earning MOC points, the question release schedule and more at www.abim.org/lka.